|
The emerging epidemiology of human
trafficking and modern slavery

Mohsen
Rezaeian
Correspondence:
Professor Mohsen Rezaeian
PhD, Epidemiologist
Epidemiology and Biostatistics Department
Occupational Environmental Research
Center
Rafsanjan Medical School
Rafsanjan University of Medical Sciences
Rafsanjan-Iran
Tel: +983431315000
Fax: +983431315003
Email: moeygmr2@yahoo.co.uk
Abstract
Although within literature human
trafficking is considered as a form
of modern slavery, it should be more
considered as a mediator for modern
slavery. The ultimate intention of
human trafficking is to capture humans
and sell them to someone who wants
to buy and abuse humans in one of
the various types of modern slavery,
for economic gain from such trade.
As a result, human trafficking should
be considered as a gross violation
of human rights which leads to modern
slavery and should be prohibited all
through the world. The aim of the
present article therefore, is to take
a fresh look at the epidemiology of
human trafficking and modern slavery.
Key words: Epidemiology; human
trafficking, modern slavery
Introduction
Within literature human trafficking
is considered as modern slavery (1)
or at the very least as a subtype
of it (2). However, in my point of
view, it should be more considered
as a mediator for modern slavery.
The ultimate intention of human trafficking
is to capture humans and sell them
to someone who wants to buy and abuse
humans in one of the various types
of modern slavery, for economic gain
from such trade. Modern slavery may
include: prostitution, sexual exploitation,
forced labor, bonded labor, forced
child labor, slavery, servitude, child
soldiering, brides and removal of
organs for economic gain (3-5).
As a result, human trafficking should
be considered as a gross violation
of human rights and a horrific crime
which leads to modern slavery and
should be prohibited all through the
world (6). In other words no one should
be allowed to enlist, convey, transfer,
harbour or receive a human being through
the use of threat, compelling or kidnapping
(3).
Evidence suggests that if efficient
prevention strategies have not been
put in place and within a short period
of time human trafficking and modern
slavery are going to exceed other
types of trafficking including arms
and drugs (7). It has been estimated
that only sex trafficking of women
and girls worth $32 billion annually.
Furthermore, the victims of human
trafficking will be abused over a
number of years being more profitable
than arms and drugs that might be
abused just once (8). Therefore, given
the soaring trend of human trafficking
and modern slavery and its profound
adverse health consequences, the aim
of the present article is to take
a fresh look at the epidemiology of
human trafficking and modern slavery.
The epidemiology
of human trafficking and modern slavery
It is highly difficult to have a real
estimate of the sheer size of human
trafficking and modern slavery in
the world. There are a number of issues
which contribute to this uncertainty.
Firstly, human trafficking mostly
occurs in those parts of the world
where law and order is disrupted due
to poverty, war, armed conflicts,
natural disasters, social unrest due
to existence of nondemocratic governments
(9).
This is not happening unintentionally
but it rather highlights a cause and
effect relationship. Poverty, unemployment,
ethnicity, gender discrimination as
the most important social determinants
are the root causes of modern slavery
(10) and in this relation, human trafficking
acts as the mediator. Moreover, manmade
disasters together with natural disasters
and due to displacement of people,
breakdown of policy and enforcement,
collapse of social cohesion could
be considered as the facilitators
(Figure 1).
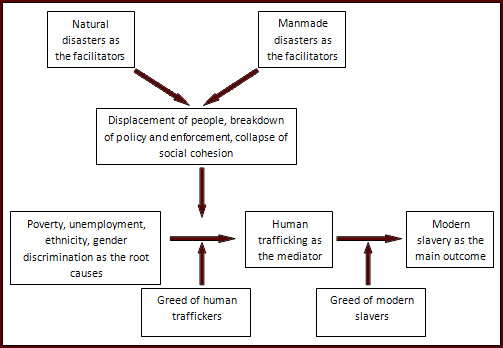
Figure 1: The relation between
poverty, unemployment, ethnicity,
gender discrimination as the root
causes and modern slavery as the main
outcome taking into consideration
the role of human trafficking as the
mediator and manmade and natural disasters
as the facilitators
In any out of law and order places
it is very difficult to gather even
straightforward data; therefore, gathering
sensitive data such as detail of human
trafficking would be rather impossible.
Secondly, there are different definitions
and connotations for human trafficking
and modern slavery making their measurement
very difficult (11). Thirdly, those
who are involved in human trafficking
either as the perpetrator and/or even
some victims while they are in captivity
chose to be silent for not being caught
by officials or due to fear and shame,
respectively. Therefore, we always
should consider underreporting and
underestimation in any human trafficking
and modern slavery reports.
Given the above discussion, the newly
published 2016 third edition of the
Global Slavery Index, by using a rather
methodological sound approach, provides
the latest estimates. Based on this
report, currently in our world there
are 45.8 million of people who live
as modern day slaves substantially
more than the 2014 estimate which
was 35.8 million enslaved people.
Fifty eight percent of 45.8 million
enslaved people are in five countries
which are India, China, Pakistan,
Bangladesh and Uzbekistan. Furthermore,
the countries with the highest prevalence
of modern slavery are: North Korea,
Uzbekistan, Cambodia, India, Qatar,
Pakistan, Democratic Republic of the
Congo, Sudan, Iraq, Afghanistan, Yemen,
Syria, South Sudan, Somalia, Libya,
Central African Republic, Mauritania,
Haiti, Dominican Republic, Myanmar
and Bangladesh (11).
A report that was published in 2014
by the United Nations Office on Drugs
and Crime reveals that across the
world and from 2010 to 2012 victims
with 152 diverse nationalities were
identified in 124 countries. Furthermore,
49%, 21%, 18% and 12% of detected
victims are adult women, girls, adult
men and boys, respectively. This report
also provides a very useful typology
on the organizations which are involved
in human trafficking. Based on this
typology we can identify three types
of organizations as follows: Firstly,
there are Small Local Operations which
are involved in short-distance trafficking
of very few people with limited profits.
Secondly, there are Medium Sub-regional
Operations which are involved in Sub-regional
trafficking of few people with higher
profits. Thirdly, there are Large
Trans-regional Operations which are
involved in long-distance trafficking
of large numbers of people with very
high profits (12).
Investigating the geographical pattern
of trans-regional trafficking reveals
that: Middle East, Western and Central
Europe, and North and Central America
and the Caribbean, are the main destinations
of this highly profitable investment.
Whilst the origins of victims seems
to be diverse and includes countries
in most other regions including: East
Asians, South Asians, Eastern and
Central Europeans, Sub-Saharan Africans
and South Americans (12) (Figure 2).

Figure 2. A map demonstrating the
major target areas of trans-regional
trafficking flows (in blue) and their
noteworthy origins, 2010-2012.
Source: UNODC, Global Report on
Trafficking in Persons 2014. (United
Nations publication, Sales No. E.14.V.10).
This map also highlights another
important and evoking issue. As it
has been mentioned earlier the origin
of trans-regional trafficking relates
to the places where law and order
is disrupted due to poverty, war,
armed conflicts, natural disasters
and social unrest due to existence
of nondemocratic governments. Nevertheless,
some of the main destinations of this
trans-regional trafficking, or the
places that modern slavery actually
happen, are places where there seems
to be law and order in place i.e.
Central Europe and North and Central
America. According to CNN in 2014
Atlanta's illegal sex industry makes
more than $290 million (13). This
trend not only explains why we should
distinguish between human trafficking
and modern slavery but it also reminds
us how difficult it would be to prevent
these social sicknesses.
The health
consequences of human trafficking
and modern slavery
Human trafficking and modern slavery
have profound physical and psychological
health consequences. This occurs because
the victims experience a vast array
of physical and mental health problems
including appalling living situations,
unsafe working circumstances, inadequate
sanitation, poor nutrition, physical
and psychological violence, and postponement
in seeking medical care (5).
Given the hidden nature of human trafficking
and modern slavery the research on
physical and psychological health
consequences of these social sicknesses
are extremely limited. This is especially
the case when people are in captivity.
Therefore, in what follows the results
of only a few most recent studies
on physical and mental health symptoms
of survivors of human trafficking
and modern slavery are reported:
The results of a study on the physical
health symptoms of 120 trafficked
women who had received post-trafficking
support in Moldova have revealed that
61.7%, 60.9% and 44.2% of them have
reported headaches, stomach pain and
memory problems, respectively (14).
A study on 387 children and adolescents
aged 10 to 17 years, survivors of
human trafficking in the Greater Mekong
Sub-region which includes Thailand,
Vietnam, Cambodia, Laos, Myanmar,
and Yunnan Province of China, revealed
that: 12% had tried to commit suicide
in the month before the interview,
56% had symptoms of depression, 33%
had symptoms of anxiety disorder,
and 26% had symptoms of posttraumatic
stress disorder (15).
In another study and by interviewing
more than 1000 people who entered
post-trafficking services in Cambodia,
Thailand, and Vietnam it has been
revealed that: 5·2% had tried
to commit suicide in the past month,
61·2% had reported symptoms
of depression, 42·8% had reported
symptoms of anxiety, and 38·9%
had reported symptoms of post-traumatic
stress disorder. Furthermore, 48%
reported physical violence, sexual
violence, or both, 47% reported to
be threatened and 20% reported to
be locked in a room. Finally, 22%
reported to have a severe injury at
work. (16).
The results of a study on the psychological
health of 66 sexually trafficked female
survivors in Nepal have highlighted
that 85·5% had reported symptoms
of depression, 87% had reported symptoms
of anxiety, and 29·7% had reported
symptoms of post-traumatic stress
disorder (17).
How to prevent
human trafficking and modern slavery
In terms of epidemiological knowledge
it would be possible to prevent any
dilemmas such as human trafficking
and modern slavery in a vast array
of prevention strategies. From primordial
and primary prevention which seek
to prevent something before it happens
to secondary and tertiary prevention
which seeks to identify the problem
and to stop its progress and complications
as soon as possible.
It is no doubt that for such profound
social sicknesses as human trafficking
and modern slavery, it would be better
to apply primordial and primary prevention
strategies. Human beings are born
free and they should have the right
to live freely. No one should gain
whatsoever the illegitimate power
to force another human being to be
a subject of modern slavery. Unfortunately
however, human trafficking and modern
slavery as inhuman social sicknesses
are happening increasingly in our
world and in front of our eyes.
We are all responsible no matter if
we work in academia, governmental
organizations, international organizations,
charities, etc. We should all stand
up and through close collaboration
make a strong coalition against such
evil phenomenon to eradicate them
once and forever. Combating the root
causes of human trafficking and modern
slavery including poverty or its facilitator
factors including wars, armed conflicts,
natural disasters, social unrest due
to existing of undemocratic governments,
etc. should be a mandate for all of
us. We also need enforcement of efficient
policies (9 & 10). It has already
been mentioned that taking this path
would be very difficult but we should
take it if we desire to protect humanity.
Furthermore, it is absolutely vital
that immediately after any natural
or manmade disasters proper attention
is paid to the needs of the vulnerable
groups such as women and children
who are separated from their family
(18). These people are more prone
to violence and trafficking. Therefore,
they should immediately be recognized
and reunited with their family or
obtain legal support from the relevant
officials (19 & 20). Unfortunately,
according to a recent report by the
Guardian at least 10,000 unaccompanied
child refugees have vanished after
arriving in Europe mostly due to the
activities of organized trafficking
syndicates (21).
For secondary and tertiary prevention
however, it seems that among all staff
of public sectors and services, health
care professionals have a major role
to play (22). As it has been discussed
earlier, human trafficking and modern
slavery have profound physical and
mental health consequences. Therefore,
it is highly likely that due to these
problems the victims are ultimately
in contact with emergency departments
and/or mental health services.
The results of a cross-sectional survey
on National Health Service (NHS) professionals
in UK has revealed that: 13% of them
reported prior contact with a patient
likely of having been trafficked,
however, 86.8% reported insufficient
awareness of what questions to ask
to recognize possible victims and
78.3% reported that they had inadequate
training to help victims of human
trafficking (23).
This explains why health service professionals
should be sufficiently trained about
how to recognize a victim of human
trafficking. Furthermore, they should
be trained on how to efficiently manage
such victims taking into consideration
the available supports. Therefore,
they should be educated on how to
competently collaborate with law enforcement
authorities and engage advocacy partners.
In order to fulfill all above educational
goals, the medical schools need to
revise their medical curriculum based
on the existing evidence and more
educational resources and textbooks
should be developed (24-26). Fortunately,
existing evidence has highlighted
how a brief training intervention
for emergency providers could largely
increase their confidence and abilities
to identify and treat a trafficked
patient (27 & 5).
Conclusion
The ultimate intention of human trafficking
is to give illegitimate power to a
human being in order to force another
human being to be a subject of modern
slavery i.e. prostitution, sexual
exploitation, forced labor, slavery,
servitude, child soldiering, brides
and removal of organs for economic
gain. As a result, human trafficking
should be considered as a gross violation
of human rights which leads to modern
slavery. Both human trafficking and
modern slavery should be eradicated
by a coalition and close collaboration
of national governments and relevant
national and international organizations.
References
1. Logan TK, Walker R, Hunt G. Understanding
human trafficking in the United States
Trauma Violence Abuse. 2009 Jan;10(1):3-30.
2. Doezema J. Loose women or lost
women? The re-emergence of the myth
of white slavery in contemporary discourses
of trafficking in women. Gender Issues.
2000 Winter;18(1):23-50.
3. United Nations Office on Drugs
and Crime (UNODC). United Nations
Convention Against Transnational Organized
Crime and the Protocols Thereto. Vienna.
2004.
4. Barrows J, Finger R. Human trafficking
and the healthcare professional. South
Med J. 2008 May;101(5):521-4.
5. Grace AM, Lippert S, Collins K,
Pineda N, Tolani A, Walker R, et al.
Educating health care professionals
on human trafficking. Pediatr Emerg
Care. 2014 Dec;30(12):856-61.
6. Ronda-Pérez E, La Parra
D. Eradicating human trafficking:
a social and public health policy
priority. Epidemiol Psychiatr Sci.
2016 Apr 18:1-2. [Epub ahead of print]
7. Wheaton EM, Schauer EJ, Galli TV.
Economics of human trafficking. Int
Migr. 2010;48(4):114-41.
8. Deshpande NA, Nour NM. Sex trafficking
of women and girls. Rev Obstet Gynecol.
2013;6(1):e22-7.
9. Rezaeian M. Challenges of developing
countries' epidemiologists in the
21st century. Acta Med Iran. 2016;
54(1):4-8.
10. Perry KM, McEwing L. How do social
determinants affect human trafficking
in Southeast Asia, and what can we
do about it? A systematic review.
Health Hum Rights. 2013 Dec 12;15(2):138-59.
11. "Global Slavery Index".
Walk Free Foundation. http://www.globalslaveryindex.org/
Retrieved 4 June 2016.
12. United Nations Office on Drugs
and Crime (UNODC). Global Report on
Trafficking in Persons 2014. Vienna.
2014.
13. CNN. Sex trafficking: The new
American slavery. http://edition.cnn.com/2015/07/20/us/sex-trafficking/.
Last accessed June 2016.
14. Oram S, Ostrovschi NV, Gorceag
VI, Hotineanu MA, Gorceag L, Trigub
C, Abas M. Physical health symptoms
reported by trafficked women receiving
post-trafficking support in Moldova:
prevalence, severity and associated
factors. BMC Womens Health. 2012 Jul
26;12:20.
15. Kiss L, Yun K, Pocock N, Zimmerman
C. Exploitation, Violence, and Suicide
Risk Among Child and Adolescent Survivors
of Human Trafficking in the Greater
Mekong Subregion. JAMA Pediatr. 2015
Sep;169(9):e152278.
16. Kiss L, Pocock NS, Naisanguansri
V, Suos S, Dickson B, Thuy D, et al.
Health of men, women, and children
in post-trafficking services in Cambodia,
Thailand, and Vietnam: an observational
cross-sectional study. Lancet Glob
Health. 2015 Mar;3(3):e154-61.
17. Rimal R, Papadopoulos C. The mental
health of sexually trafficked female
survivors in Nepal. Int J Soc Psychiatry.
2016 Jun 3. pii: 0020764016651457.
[Epub ahead of print]
18. Rezaeian M. The association between
natural disasters and violence: a
systematic review of the literature
and a call for more epidemiological
studies. J Res Med Sci 2013;18:1103-7.
19. Pittaway E, Bartolomei L, Rees
S. Neglected issues and voices. Asia
Pac J Public Health 2007;19:69.
20. Brandenburg MA, Watkins SM, Brandenburg
KL, Schieche C. Operation Child-ID:
Reunifying children with their legal
guardians after Hurricane Katrina.
Disasters 2007;31:277-87.
21. The Guardian. 10,000 refugee children
are missing, says Europol. http://www.theguardian.com/world/2016/jan/30/fears-for-missing-child-refugees.
Last accessed June 2016.
22. O'Callaghan MG. The health care
professional as a modern abolitionist.
Perm J. 2012 Spring;16(2):67-9.
23. Ross C, Dimitrova S, Howard LM,
Dewey M, Zimmerman C, Oram S. Human
trafficking and health: a cross-sectional
survey of NHS professionals' contact
with victims of human trafficking.
BMJ Open. 2015 Aug 20;5(8):e008682.
24. Stoklosa H, Grace AM, Littenberg
N. Medical education on human trafficking.
AMA J Ethics. 2015 Oct 1;17(10):914-21.
25. Domoney J, Howard LM, Abas M,
Broadbent M, Oram S. Mental health
service responses to human trafficking:
a qualitative study of professionals'
experiences of providing care. BMC
Psychiatry. 2015 Nov 17;15:289.
26. Ahn R, Alpert EJ, Purcell G, Konstantopoulos
WM, McGahan A, Cafferty E, et al.
Human trafficking: review of educational
resources for health professionals.
Am J Prev Med. 2013 Mar;44(3):283-9.
27. Chisolm-Straker M, Richardson
LD, Cossio T. Combating slavery in
the 21st century: the role of emergency
medicine. J Health Care Poor Underserved.
2012 Aug;23(3):980-7.
|
